
AI in Healthcare Modeling: A Practical Perspective in Today’s Industry
An emerging question in the field of health economics and outcomes research (HEOR) is, what happens when healthcare models move from mechanistic equations that we can interpret to black-box, data-driven systems that are used to inform healthcare decisions worth billions of dollars?
To avoid this risk, we must continue to stress human oversight of artificial intelligence (AI), especially in fields like healthcare, where patient outcomes depend on the choice of value frameworks, rigorous data-driven mathematical modeling, and effective communication of results to stakeholders.
The Evolution of Mathematical Modeling for Healthcare
Health economic modeling first emerged in the 1970s with the development of decision-analytic models designed to determine the value of healthcare technologies. These approaches were influenced by earlier mechanistic modeling traditions, particularly those used in infectious disease dynamics. These mechanistic models trace their origins to the start of 20th century, when scientists like Ronald Ross and his collaborators first used differential equations to describe disease transmission.
However, the role of real-world data (RWD) in healthcare research expanded significantly in the early 2000s, when electronic health records, insurance claims databases, and patient registries became increasingly available. These large datasets allowed researchers to study treatment outcomes in real-world populations rather than relying solely on controlled clinical trials. Today, these datasets are the backbone of many health economic models, providing key inputs and enabling uncertainty quantification.
At the same time, the scale, heterogeneity, and complexity of these data created a demand for new analytical approaches, thereby creating an environment in which machine learning (ML) and AI could contribute meaningfully to healthcare analysis. Although privacy and ethical concerns limited their use for many years, recent advances in data governance, computing infrastructure, and AI methods have enabled broader applications of AI and ML in healthcare research.
Public health crises over the past two decades have further highlighted both the value and limitations of mathematical models. The 2001 Sept. 11 attacks and subsequent anthrax incidents in the U.S. led to the establishment of new multidisciplinary modeling initiatives and task forces to strengthen preparedness for biological threats in the U.S. The increased focus and investment in infrastructure led to a surge in the development and application of mathematical models, which were used in response and preparedness efforts during the 2009 H1N1 influenza pandemic (commonly known as swine flu), the Ebola and Zika virus outbreaks, and most recently the COVID-19 pandemic. However, these crises also unveiled the challenges of uncertainty, data quality, and communication that arise when models are used in real-time decision making.
AI in Modern Healthcare
Today, AI is rapidly transforming healthcare modeling within HEOR. Health economic models quickly became central tools in cost-effectiveness analysis, budget impact analysis, and value assessment of healthcare technologies such as pharmaceuticals, vaccines, medical devices, procedures, and digital health applications. These models can assess health technology value across different stages of a product’s lifecycle [4] by combining clinical evidence, epidemiological data, and economic outcomes to estimate how different value drivers influence its long-term impact [6].
However, the transition from traditional mathematical modeling to AI-enabled systems is not simply a matter of replacing equations with algorithms. The real challenge is learning how to integrate AI carefully into existing modeling frameworks while preserving interpretability, transparency, and decision relevance. Healthcare modeling projects typically follow several practical stages:
- Identify the decision question and demonstrate to potential clients why a model is needed to generate new evidence supporting their product or intervention. This often involves targeted literature reviews and evidence synthesis using AI tools such as Elicit, Consensus, or NotebookLM to identify relevant studies and input parameter ranges.
- Develop a modeling protocol and conceptual framework. Evidence for the model may come from clinical trials, observational studies, electronic health records (EHRs), insurance claims databases, disease registries, surveillance systems, or hospital chargemaster data.
- Construct a transparent conceptual model that reflects clinical pathways and relevant economic outcomes associated with the intervention. This step also requires literature review, but of modeling studies.
- Computational implementation of the model, often using tools such as Excel, R, or Python, and systematic analysis using client-friendly platforms (such as Dashboards) that allow stakeholders to understand the structure and the analysis. Generative AI systems such as ChatGPT and Gemini are often used to assist with coding of model, scenario analysis, sensitivity analysis, and exploratory data analysis.
- Document assumptions, the modeling choices, evidence sources, and results in technical reports used to support regulatory, reimbursement, or policy decisions.
Historically, healthcare modelers used differential or discrete equation models to describe disease transmission dynamics; Markov models to simulate disease progression and treatment pathways; decision trees to capture short-term clinical decisions; and survival models to evaluate patient outcomes over time [2]. While these approaches remain essential because they encode biological, clinical, and economic knowledge in transparent mathematical structures, AI methods introduce new capabilities.
AI tools can provide high-level pattern recognition, high-dimensional data analysis, automated evidence extraction, and rapid code generation; however, without careful design these methods can produce black box models that are difficult to validate or interpret. For healthcare decision-making, where models may inform regulatory approvals, reimbursement policies, and clinical guidelines, transparency remains critical. Hence, the most productive path is not purely mechanistic modeling nor purely data-driven AI, instead, hybrid modeling systems that combine both approaches creatively offer the greatest potential.
Digital Twins
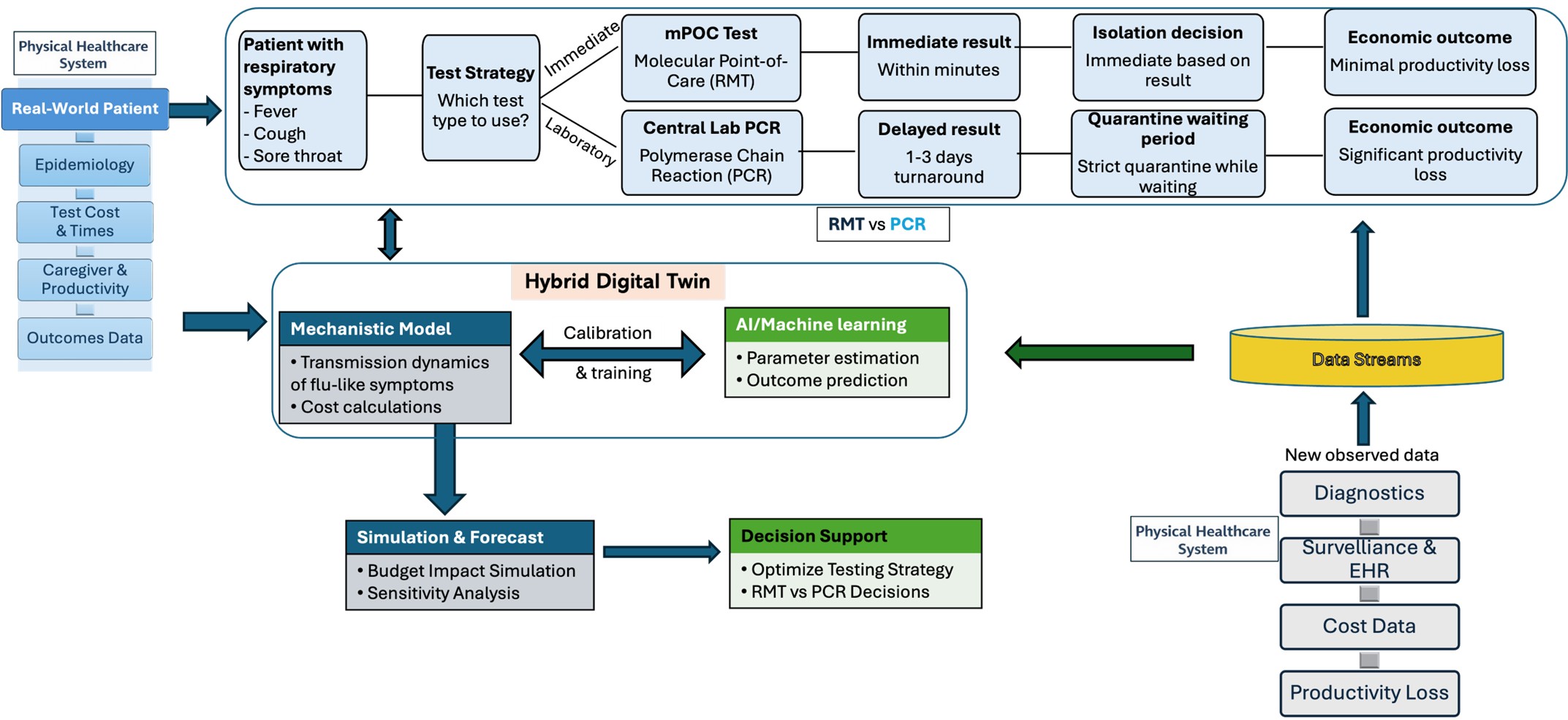
This hybrid philosophy is particularly important in the emerging field of digital twins in healthcare. Digital twins attempt to represent evolving patient or population states through computational models that continuously integrate new data. When digital twins rely entirely on ML algorithms trained on historical data, they may perform well during development but struggle when clinical conditions change or new treatments emerge. Hybrid digital twins combine mechanistic disease models with data-driven learning components, allowing researchers to incorporate biological knowledge while still adapting to RWD streams.
In cardiovascular studies, propensity score matching—one of the widely used methods for estimating treatment effects from observational data—helps researchers account for confounding factors; ML models can identify nonlinear interactions or patient subgroups that may benefit most from specific therapies. Similarly, structural equation modeling remains an important framework for studying complex psychosocial relationships, such as how stress, social environment, and behavioral factors contribute to burnout. AI methods can assist in psychological research settings by identifying latent patterns in large datasets and supporting variable selection. In oncology research, random survival forest models extend traditional survival analysis by allowing flexible modeling of high-dimensional genomic data, helping identify genetic markers associated with breast cancer prognosis while still incorporating survival-time outcomes[3]. These examples show how AI can complement, rather than replace, classical statistical methodologies in healthcare research.
Healthcare Modeling with AI and Agentic Systems
AI is also transforming how healthcare models are communicated to decision makers. Increasingly, organizations rely on interactive dashboards and decision-support platforms that integrate modeling results with real-world evidence and economic data. In earlier work on the Siddhi analytical platform, modeling results were embedded into dashboards that allowed stakeholders to explore scenarios dynamically rather than relying solely on static reports [1]. AI can enhance these systems by automating data ingestion, detecting emerging patterns in clinical or financial datasets, and generating scenario analyses in real time.
The workflow of healthcare modeling has also transformed due to AI-enabled research tools such as Connected Papers, used for visualizing relationships among scientific publications; Zotero, a citation management system that supports organized literature management; and Julius AI, used for rapid visualization of insights from preliminary data analysis. Generative AI systems such as ChatGPT, Claude, and Gemini, can assist with literature synthesis, conceptual exploration, and code prototyping. However, they should augment, not replace, rigorous modeling practices and human oversight [8].
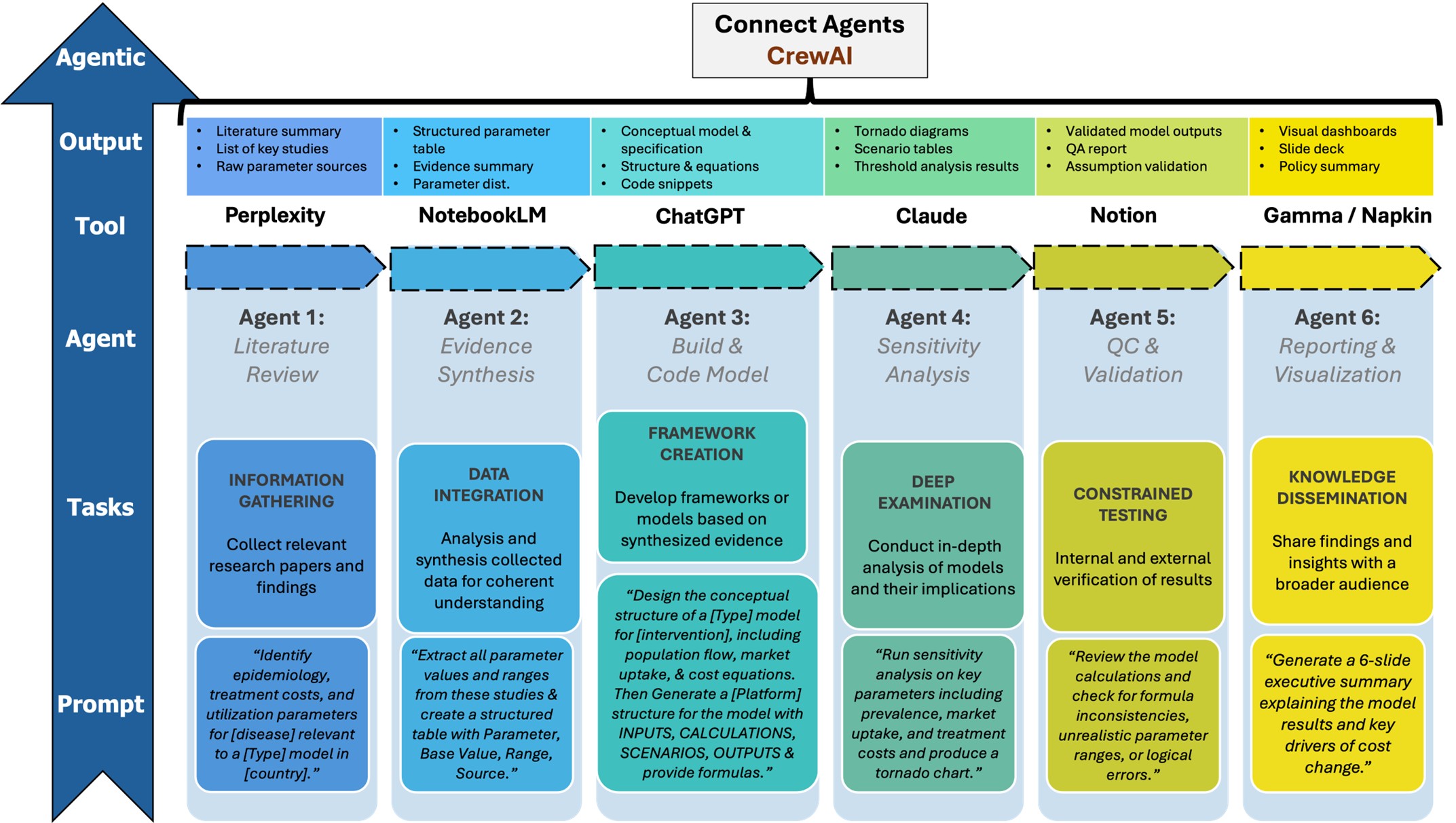
A particularly important emerging development is agentic AI, in which multiple specialized AI agents perform coordinated tasks across different stages of a modeling project. Rather than relying on a single AI tool, agentic workflows organize multiple AI systems into a structured pipeline that mirrors how research teams operate and form a living health technology assessment. For example, in health economic modeling projects that evaluate diagnostic strategies, such as sequential molecular point-of-care testing for COVID-19 and influenza compared with central laboratory polymerase chain reaction testing [5], an agent-based workflow could automate literature review, evidence synthesis, parameter extraction, and sensitivity analysis generation. Such systems do not replace human expertise but can function as supervised assistants that accelerate routine analytical tasks while allowing modeling experts to focus on conceptual design and interpretation. A simplified agentic workflow might include:
- Research Agent (e.g. Perplexity) — responsible for identifying relevant literature and parameter ranges.
- Evidence Synthesizer (e.g. NotebookLM) — used to extract parameters and summarize studies.
- Model Architect (e.g. ChatGPT or Claude) — defines model logic, equations, and assumptions as well as generates model code or Excel implementation and/or R snippets.
- Sensitivity Agent (e.g. ChatGPT or Claude) — performs one-way sensitivity analysis, probabilistic sensitivity analysis, and break-even analysis.
- Program Agent (e.g. Notion) — can perform quality control analysis, validate results, and organize project documentation and workflow management.
- Storytelling Agent (e.g. Gamma or Napkin) — produces visualizations and creates slide deck presentation materials.
Another emerging development is the use of agent orchestration frameworks that coordinate multiple AI agents working together on complex analytical tasks. For example, a modeler can use CrewAI, which can define agents such as literature retrieval, parameter extraction, model specification, code generation, testing, and documentation, within a structured workflow. For more technically complex workflows that require explicit control over workflow state and decision branching, LangGraph could be used for defining graph-based agent interactions, or Google Antigravity—an agent-first integrated development environment—could be useful in coordinating autonomous coding agents within larger software systems. These agentic tools are assistive and can improve productivity and traceability, but still require careful human oversight, validation protocols, and governance for reliable healthcare modeling.
For early career applied mathematicians considering careers in healthcare modeling, several lessons emerge from this evolving landscape:
- Strong mathematical foundations are critical, including knowledge of probability theory, statistical inference, optimization, and dynamical systems.
- Successful researchers must develop domain knowledge in epidemiology, health economics, and/or clinical research methods.
- The ability to work with RWD, which is often incomplete, noisy, and biased, is increasingly important.
- Communication skills are as important as technical skills, as healthcare models ultimately inform decisions made by clinicians, regulators, and policymakers.
The most important realization is that healthcare modeling is fundamentally a socio-technical discipline, that is, models do not exist in isolation; they are embedded within healthcare systems, regulatory environments, and organizational decision processes. AI tools can accelerate analysis and improve productivity, but they cannot replace careful judgment about data quality and standardization across sources, product-specific modeling assumptions, client-specific decision contexts, and broader ethical considerations.
In the future, healthcare modeling will likely evolve into an ecosystem where hybrid models, AI-assisted workflows, and domain expertise work together. Applied mathematicians who can bridge theoretical modeling, data science, and practical decision support will play a crucial role in shaping how AI is responsibly used in healthcare.
References
[1] Moinudeen, S.A.K., Nithiyavathani, A., Keerthan, R.M., Mubayi, A., Ramesh, S., Harshitha, S., & Kachroo, K. (2023). SIDDHI: An Easy-to-use Web-based Trailblazing Software Tool for Developing Data-Driven Health Economics Models and Performing Cost-Effectiveness Analysis. Int. J. Health Technol. Innov., 4(3), 56-64.
[2] Mubayi, A., Mubayi, A., & Akman, O. (2024). The Shifting Nature of Health and Economic Evaluations of Disease Interventions. SIAM News Online. Retrieved from: https://www.siam.org/publications/siam-news/articles/the-shifting-nature-of-health-and-economic-evaluations-of-disease-interventions/.
[3] Mubayi, A., Ghosh, S., & Grilo, L.M. (2023). Exploring Statistical Relationships for Risk Assessment and Value Computation of Digital Health Technologies in India. Int. J. Health Technol. Innov., 4(2), 5-11.
[4] Shafrin, J., Kim, J., Cohen, J.T., Garrison, L.P., Goldman, D.A., Doshi, J.A., … Willke, R. (2024). Valuing the Societal Impact of Medicines and Other Health Technologies: A User Guide to Current Best Practices. Forum for Health Economics & Policy, 27(1), 29–116.
[5] Shafrin, J., Mubayi, A., Birch, K., Land, N., Sotak M., Venkatachalam, M., … Ayad, M. (2022). Economic Value of Sequential Molecular Point-of-Care Testing for COVID-19 and Influenza vs. Central Laboratory PCR. [Poster presentation] ISPOR Annual Meeting.
[6] Sanders, G.D., Neumann, P.J., Basu, A., Brock, D.W., Feeny, D., Krahn, M., … & Ganiats, T.G. (2022). Recommendations for Conduct, Methodological Practices, and Reporting of Cost-effectiveness Analyses: Second Panel on Cost-Effectiveness in Health and Medicine. JAMA, 16(10):1093-1103.
[7] M. Nadeem, M., Kostic, S., Dornhöfer, M., Weber, C., & Fathi, M. (2025). A comprehensive review of digital twin in healthcare in the scope of simulative health-monitoring. Digital Health, 11.
[8] Ye, Y., Pandey, A., Bawden, C., Sumsuzzman, D.M., Rajput, R., Shoukat, A., … Galvani, A.P. (2025). Integrating artificial intelligence with mechanistic epidemiological modeling: a scoping review of opportunities and challenges. Nat. Comm., 16(1), 581.
About the Authors
Anuj Mubayi
Principal, NumericaIQ
Anuj Mubayi is the Principal of NumericaIQ, a Fellow in Residence at the Intercollegiate Biomathematics Alliance in the USA, an honorary fellow at the Kalam Institute of Health Technology in India, and a Scientific Advisor for Kalam Experts. Previously, Mubayi served as director of the Mathematical and Theoretical Biology Institute, was a faculty member at Arizona State University, and worked in the healthcare industry. His expertise spans health decision science, with a focus on health economics, data-driven disease modeling, and real-world evidence generation.

Anamika Mubayi
Director, Kalam Experts
Anamika Mubayi is director at Kalam Experts, a data analytics and consulting company supporting medical device and healthcare digital technology companies based in India. She is also a physical chemist with expertise in nanomaterials, analytical chemistry, and advanced materials characterization for emerging technology applications. Mubayi holds a Ph.D. from the University of Allahabad and an master’s from the University of Iowa. Previously, she served as Scientist-D at the International Centre for Medical Glass Engineering (IMAGE), an associate professor at Marwadi University, and project scientist at IIT Kanpur’s National Centre for Flexible Electronics. Her work bridges science, materials research, and healthcare technology innovation.


Stay Up-to-Date with Email Alerts
Sign up for our monthly newsletter and emails about other topics of your choosing.
