
Dynamic Left Atrium Model Sheds Light on Supraventricular Tachycardia
Supraventricular tachycardia (SVT) is an irregular heart rhythm disorder that is a significant contributing factor to stroke, heart failure, and—in some cases—acute myocardial infarction (i.e., heart attack): several of the leading causes of death worldwide [3, 4]. In our pursuit of a future that is free from cardiovascular disease and stroke, it is therefore imperative to reduce the occurrence of SVT.
SVT includes all cardiac arrhythmias wherein the abnormal electrical activity originates above the ventricles. This type of disrupted heartbeat can interfere with the natural synchronization of the atria and ventricles, disturbing laminar blood flow and causing stagnation in the small, finger-like appendages of the left atrium. This stagnation can lead to the formation of potentially lethal blood clots known as mural thrombi that may dislodge and travel to the brain or coronary arteries, resulting in heart attack or stroke. This mechanism contributes to the five-fold increase in stroke risk for individuals with atrial fibrillation.
In a healthy heart, the sinus node acts as a pacemaker by consistently generating electrical impulses that maintain a steady rhythm and rate. These impulses trigger a chain reaction that propagates through the heart and produces life-sustaining contractions. However, ectopic impulses—i.e., electrical signals that arise at the wrong place or time—can disrupt this process, causing the atria to flutter, beat out of sync with the ventricles, or exhibit other dysfunctional patterns.
In many cases, patients can effectively manage SVT with lifestyle modifications and medication [2, 3]. But some drugs are difficult for patients to tolerate, and the most effective ones may be hepatotoxic, leading to serious side effects. As a result, catheter ablation—although more invasive than drug therapy—has proven to be the safest and most reliably effective option for patients with recurrent SVT [1].
Radiofrequency catheter ablation and three-dimensional electroanatomic mapping techniques have improved dramatically over the past decade, allowing physicians to perform complex procedures on beating hearts — a feat that was once thought to be impossible. Nonetheless, the origins of arrhythmias and the optimal treatment strategies with radiofrequency ablation are still relatively unknown. Clinicians, researchers, and medical students would greatly benefit from a method to rapidly and affordably test hypotheses and observe outcomes.
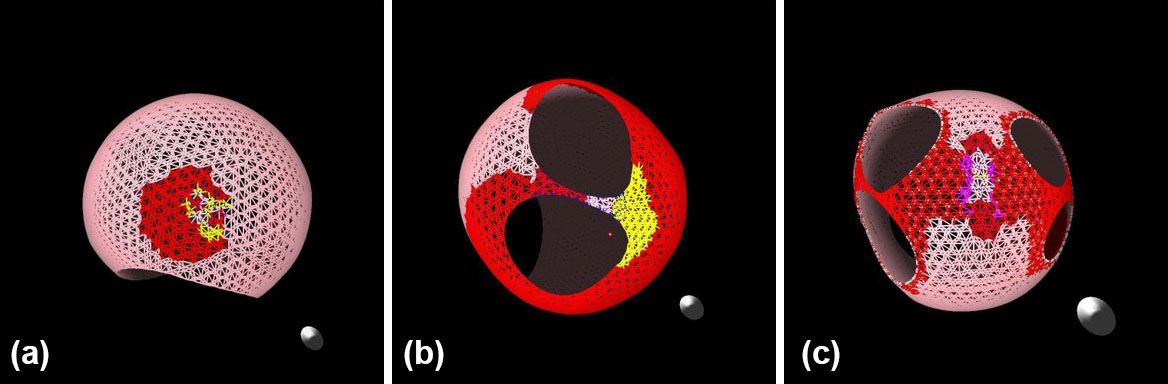
Real-time maps of cardiac electrical activity are merely visualizations, not functional models that are capable of testing ideas. The models that do exist are either too slow or not adequately interactive. To address this insufficiency, we developed an interactive computer model of the left atrium that runs in near-real time. Our model [5] enables users to simulate left atrium tissue substrates, where arrhythmias may arise spontaneously or be induced via strategically placed ectopic events (see Figure 1). Simulated ablations can then terminate these arrhythmias. This tool allows researchers and electrophysiologists to explore and refine ablation strategies outside of the operating room, potentially improving patient outcomes and saving lives.
We focus on the left atrium because that is where most complex arrhythmias originate. Users can manipulate our model—which captures both electrical and mechanical activity—at the individual muscle level (where “muscle” refers to a group of cardiomyocytes) and introduce ectopic events. The model represents cardiac tissue as a network of nodes and connectors; nodes carry the tissue’s mass and spatial properties, while connectors manage the force between nodes and transmit electrical signals. Each node is a point mass that tracks position, mass, connected elements, and activation state (where “off” indicates ablated tissue). Connectors are massless Hookean springs that act as timed signal conductors; every connector has an internal clock to manage its processes, tracking its resting and contraction parameters as well as signal velocity and direction.
The entire model functions as a sparsely connected \(N\)-body simulation that we advance in time via leapfrog integration. Users can efficiently optimize simulations to run on parallel hardware, such as NVIDIA graphics processing units (GPUs). We developed and tested the current software on a workstation with an NVIDIA RTX A6000 GPU, then demonstrated it to medical professionals on a laptop with an NVIDIA GTX 3080 GPU. The code is lightweight and does not require high-end hardware, which ensures accessibility for researchers without necessitating access to a supercomputing facility.
The core codebase is written in C and C++, with performance-critical components written in CUDA and offloaded to the GPU for acceleration. We modeled the left atrium’s anatomical structure—including its nodes and connectors—with Blender, and used OpenGL to develop the graphical interface.
In conclusion, we must address the burden of SVT to reduce the global impact of cardiovascular disease and stroke. Our interactive, near-real-time model of the left atrium is a powerful, accessible tool with the potential to advance the understanding and treatment of cardiac arrhythmia. By combining electrical and mechanical simulation with customizable tissue properties, this model provides clinicians, researchers, and educators with a unique platform to test hypotheses, refine ablation strategies, and train future electrophysiologists. As we continue to enhance and validate the model, we hope that it will bridge the gap between theory and practice — ultimately leading to more effective patient-specific interventions and improved outcomes in cardiac care.
Bryant Wyatt delivered a minisymposium presentation about this research at the 2025 SIAM Conference on Computational Science and Engineering, which took place in Fort Worth, Texas, this past March.
References
[1] American Heart Association. (2024). Ablation for arrhythmias. Health Topics. Retrieved from https://www.heart.org/en/health-topics/arrhythmia/prevention--treatment-of-arrhythmia/ablation-for-arrhythmias.
[2] Cedars-Sinai Medical Center. (2025). Supraventricular tachycardia. Health Library. Retrieved from https://www.cedars-sinai.org/health-library/diseases-and-conditions/s/supraventricular-tachycardia.html.
[3] Mayo Clinic. (2024). Supraventricular tachycardia. Diseases & Conditions. Retrieved from https://www.mayoclinic.org/diseases-conditions/supraventricular-tachycardia/symptoms-causes/syc-20355243.
[4] National Institutes of Health. (2025). Heart disease and stroke. NIH…Turning Discovery Into Health. Retrieved from https://www.nih.gov/about-nih/nih-turning-discovery-into-health/our-biggest-health-challenges/heart-disease-stroke.
[5] Wyatt, B., Campbell, A., McIntosh, G., Little, M., & Wyatt, B. (2023). Modeling supraventricular tachycardia using dynamic computer-generated left atrium. Preprint, medRxiv.
About the Author
Bryant Wyatt
Professor, Tarleton State University
Bryant Wyatt is a professor of mathematics at Tarleton State University. He established Tarleton’s High-Performance Computing Lab with support from NVIDIA, developing it into a leading hub for interdisciplinary research that has led to numerous awards and recognition across a variety of fields. In 2018, he was named the Mathematical Association of America’s Distinguished University Teacher for the state of Texas.

Stay Up-to-Date with Email Alerts
Sign up for our monthly newsletter and emails about other topics of your choosing.
