
The Details Are in the Dosing: Modeling Efficacy-toxicity Relationships in Cancer Therapy
Despite ongoing advances in therapeutics, cancer remains a significant cause of morbidity and mortality worldwide. This persistence is due to both limited efficacy of available treatments for advanced cancers and therapy-related toxicities that restrict their use. The balance between an effective cancer therapeutic and its negative side effects is a central problem in drug development and translational research. In clinical practice, dose and schedule adjustments are made to limit preventable toxicities, but not all possible schedules, dosages, and drug combinations can be tested in vivo, much less in clinical trials. As such, there is an ongoing and critical need for robust models of cancer therapies that balance efficacy and toxicity and are applicable in the evolving landscape of cancer therapeutics. Such models require continued collaboration between mathematicians, biologists, data scientists, and clinicians.
Pharmacokinetics and Pharmacodynamics
Researchers typically model the dose-response relationship when a drug \(A\) is given at concentration \([A]\) as a Hill equation, where \(EC_{50}\) is the concentration of \(A\) to achieve \(50\) percent efficacy and \(n\) is the Hill coefficient
\[\frac{E}{E_{max}}=\frac{[A]^n}{[A]^n + EC_{50}^n}. \tag1\]
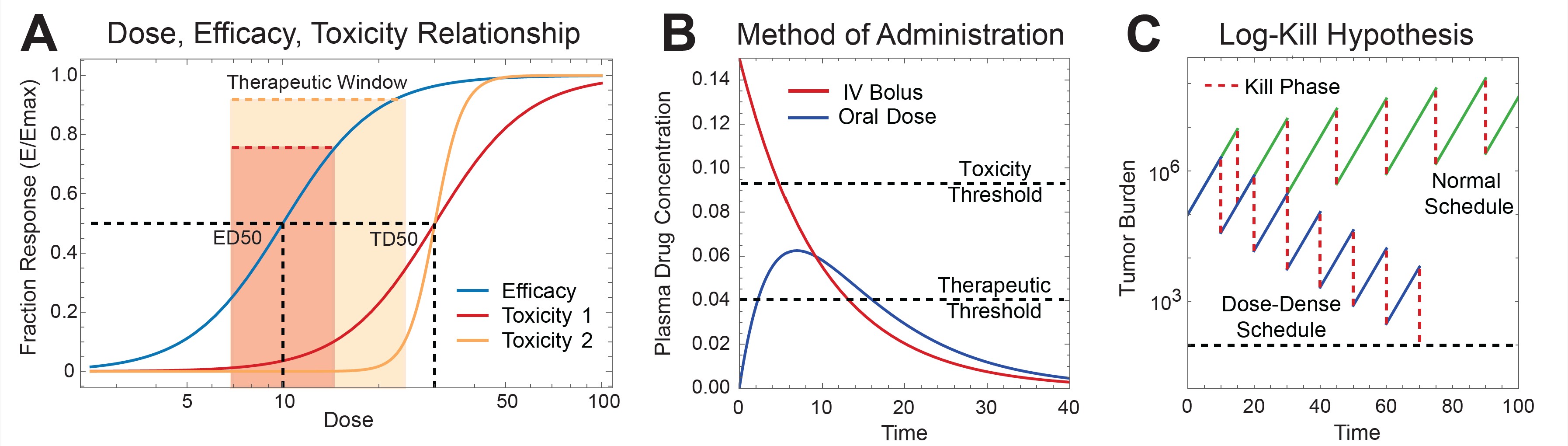
When defining clinical dosing and toxicity, we consider a related value \(ED_{50}\): the median effective dose for \(50\) percent of the population to respond to the drug in question. Similarly, \(TD_{50}\) is the dose that produces toxicity in half of the population. Scientists commonly use two metrics to describe the relationship between \(TD_{50}\) and \(ED_{50}\): the therapeutic index (TI), which is defined as \(\textrm{TI} = \frac{TD_{50}}{ED_{50}}\), and the therapeutic window, which is the range of doses in which a drug is effective before causing a predefined level of toxicity. Figure 1a illustrates two toxicity curves with the same therapeutic index but different therapeutic windows.
The relationship between the dose of drug that is delivered to a tissue and the dose of drug that is given to a patient adds another level of complexity. For a single intravenous (IV) drug dose in its activated form, a model for drug concentration over time is given by
\[\frac{dC_{iv}}{dt}=-k_eC_{iv}(t)\qquad \qquad \qquad C_{iv}(0)=D_{iv}/V_d. \tag2\]
The initial drug concentration \((C_{iv}(0))\) is the delivered dose \((D_{iv})\) divided by the volume of a drug’s distribution \((V_d).\) \(C_{iv}\) decays with rate \(k_e\) based on drug metabolism and elimination. When given in its activated form, an orally administered drug requires absorption \((k_a)\) and depends on bioavailability \((F)\) prior to elimination. In the following equations, \(D(t)\) is the amount of drug in the intestinal system and \(C(t)\) is the drug’s plasma concentration:
\[\begin{eqnarray} \frac{dD}{dt}&=&-k_aD(t) \qquad \qquad \qquad \qquad D(0)=D_oF \tag3 \\\\ \frac{dC}{dt}&=&\frac{k_a}{V_d}D(t)-k_eC(t) \tag4 \end{eqnarray}\]
Because the method of administration affects the shape of a drug’s plasma concentration, the maximum plasma-drug concentration of an oral versus an IV drug can differ significantly despite similar time above the therapeutic threshold (see Figure 1b). This discrepancy can contribute to differences in toxicity. Individual variations in drug absorption, metabolism, and excretion among patients can also lead to variability in drug exposure, even when individuals receive the same dose. Such variations can be genetic or acquired.
The use of mathematical models of drug kinetics to individualize drug dosing dates back to the 1960s and remains an active area of research. Now coined model-informed precision dosing (MIPD), pharmacokinetic models continue to maintain their relevance in oncology and are hypothesized to reduce toxicity and improve efficacy of cancer therapeutics [1]. MIPD research is interdisciplinary and requires specific models for each drug and drug combination, which makes it an attractive and relevant field for mathematicians who wish to engage in translational work.
Continuous Versus Intermittent Dose Efficacy-toxicity Relationships
Although classical models of pharmacodynamics remain central to drug discovery, we need models that can account for tumor growth and prolonged treatment periods to fully understand the efficacy and toxicity of cancer therapeutics. Cancer therapy is only considered to be effective if it can achieve tumor shrinkage or prevent growth over the course of a treatment schedule. To do so, practitioners may utilize multiple interspersed doses (intermittent therapy) or ongoing continuous doses (for example daily oral doses) aimed at achieving a steady state concentration of drug (continuous therapy).
Pioneering work on cancer growth and killing dynamics in mice [7] yielded the log-kill hypothesis of chemotherapy (see Figure 1c). In this model, cancer cell populations grow exponentially and are killed as a fraction of the initial population. A treatment is effective if it successfully shrinks the cell population below a specified level (population extinction). The model predicts that dose-dense intermittent chemotherapy regimens—wherein patients receive the same cumulative drug dose with shortened inter-dose intervals—will result in a higher probability of extinction (see Figure 1c). Consistent with this hypothesis, dose-dense regimens in breast cancer have shown improved recurrence rates [3].
Although the log-kill hypothesis is a useful tool for modeling exponential growth of hematologic malignancies, solid tumors display sigmoidal growth. To account for this difference, the Norton-Simon model incorporates density-dependent growth inhibition in the form of Gompertzian growth [5] and has predicted more effective clinical treatment schedules in solid tumors [6]. For dosing regimens that lead to log-kill or Norton-Simon dynamics, minimizing drug toxicity while maximizing efficacy is an attractive application for classical control theory approaches and an active area of mathematical research. An early example is the 1977 work of George Swan and Thomas Vincent that describes an optimal control problem based on experimental data in multiple myeloma [8]. Their model aimed to minimize patients’ total cumulative doses and the time that it takes to decrease the cancer cell population below a certain threshold. The duo predicted that continuous application of varying doses of a drug—rather than intermittent application of high doses—would lessen both toxicity and the required time for disease eradication.
Researchers have clinically explored the effects of continuous versus intermittent dosing in the context of doxorubicin, a widely used chemotherapy drug that is known to cause early and late cardiotoxicity. Scientists hypothesize that early toxicity is related to peak plasma concentration, thus making continuous infusion the obvious approach to maintain total cumulative dose while decreasing the maximum drug concentration. While continuous infusion has reduced cardiac toxicity in clinical trials, further studies are needed [9]. Because late cardiotoxicity in the form of heart failure has a nonlinear relationship with cumulative dose [10], clinical practice guidelines now recommend minimizing the lifetime cumulative dose of doxorubicin that a patient receives. This example underscores the fact that a single drug can have multiple timescales and pharmacodynamic profiles for one type of toxicity (heart failure) and highlights the need for mathematical modeling of dosing paradigms that provide insight into drug efficacy and toxicity.
Minimization of Toxicity in Adaptive Therapy
For advanced cancers where the goal of treatment is to delay progression, the minimization of treatment-related toxicity is critical. Adaptive therapy is a dosing-based approach that seeks to delay tumor progression while minimizing cumulative drug dose. This method assumes that when drug-resistant cells are already present in a tumor, therapeutic depletion of a competing drug-sensitive cell population accelerates resistant population outgrowth [2, 11]. Under this hypothesis, maintaining a portion of the sensitive cell population via careful administration of a drug and monitoring of tumor size may inhibit growth of resistant cells and delay disease progression. The following is a generalized mathematical model for intermittent adaptive therapy that assumes logistic growth of a tumor and competition between the sensitive cell population \((x)\) and resistant cell population \((y)\) [4]:
\[\begin{eqnarray} \frac{dx}{dt}&=&{r_x}x(t)(1-x(t)-{\alpha}y(t)) +{K_A}(t)h(x,{r_d}) \qquad \qquad \qquad &\textrm{sensitive cell population}& \tag5 \\\\ \frac{dy}{dt}&=&{r_y}y(t)(1-y(t)-{\beta}x(t)) \qquad \qquad \qquad &\textrm{resistant cell population}.& \tag6 \end{eqnarray}\]
Here, \(K_A\) is an indicator function that takes the value \(1\) when the drug is applied and \(0\) when it is not. Additionally, \(h(x,{r_d})\) is the effect of dose \(r_d\) on the sensitive cell population, and \(\alpha\) and \(\beta \) reflect competition terms between cell populations. Researchers have employed similar mathematical models of intermittent adaptive therapy for prostate cancer to guide clinical trials where prostate-specific antigen (PSA) serves as a surrogate for tumor size [11]. For the study, the drug was given \((K_A = 1)\) when PSA reached a certain upper threshold and withdrawn \((K_A = 0)\) when PSA reached a certain lower threshold. Under specific conditions, mathematical models of adaptive intermittent therapy have shown resistant cell population extinction where fixed dose schedules fail due to resistant outgrowth [4] (see Figures 2a and 2b).
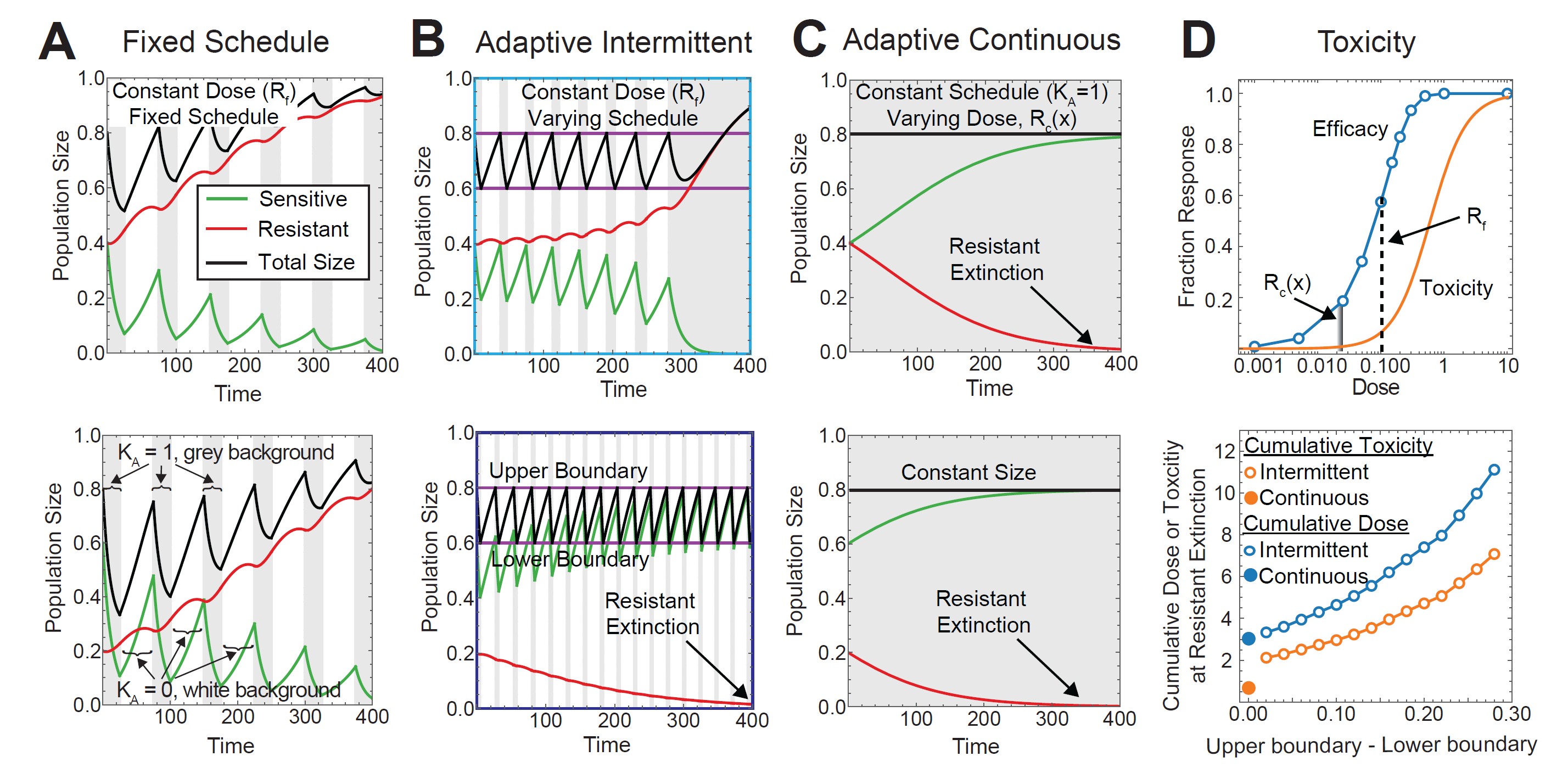
An alternative adaptive dosing regimen called continuous adaptive therapy aims to maintain a constant total tumor volume through dose modulation. We can compute this regimen in the above system by solving for a continuously applied dosing function \({{\hat{R}}_c}(x),\) which maintains a constant tumor size (see Figure 2c). We recently showed that it is possible to analytically achieve direct comparison between continuous adaptive therapy and intermittent adaptive therapy by examining the limiting behavior as the lower boundary of intermittent adaptive therapy approaches the upper boundary. Continuous adaptive therapy minimizes key properties of intermittent adaptive therapy, such as total cumulative dose and time to resistant extinction. However, total toxicity—when modeled as a convex function of dose—does not converge and is strictly minimized with continuous therapy [4] (see Figure 2d). The absolute minimization of drug toxicity despite convergence of cumulative dose stems from nonlinearity between dose and toxicity and is likely a feature of other adaptive and nonadaptive therapy models that compare continuous and intermittent dosing.
Conclusions and Opportunities
Medicine is often a landscape of examples and counterexamples rather than immutable rules, and cancer is no exception. We now know that every subtype of cancer—as well as every individual’s cancer—is unique. Within this uniqueness, even a single tumor may have diverse cell types that carry out varying molecular programs that impact drug response. Cancer therapies have mirrored this complexity with novel targets, combinations, and delivery mechanisms that can affect drug kinetics, efficacy, and toxicity. For example, immune checkpoint inhibitors—a new set of anticancer therapies that activate the body’s immune system—have the rare but serious side effect of cardiotoxicity in the form of myocarditis and complex pharmacodynamics and pharmacokinetics. This level of diversity in tumors and therapies provides ample opportunities for mathematicians to work with biologists and clinicians to develop and test a wide array of mathematical tools that can guide drug dosing and treatment schedules.
Cordelia McGehee delivered a minisymposium presentation on this research at the 2024 SIAM Conference on the Life Sciences, which took place in Portland, Ore., in June 2024.
Acknowledgments: The author would like to thank Yoichiro Mori and Scott Kaufmann for their valuable feedback.
References
[1] Darwich, A.S., Polasek, T.M., Aronson, J.K., Ogungbenro, K., Wright, D.F.B., Achour, B., … Rostami-Hodjegan, A. (2021). Model-informed precision dosing: Background, requirements, validation, implementation, and forward trajectory of individualizing drug therapy. Annu. Rev. Pharmacol. Toxicol., 61, 225-245.
[2] Gatenby, R.A., Silva, A.S., Gillies, R.J., & Frieden, B.R. (2009). Adaptive therapy. Cancer Res., 69(11), 4894-4903.
[3] Gray, R., Bradley, R., Braybrooke, J., Liu, Z., Peto, R., Davies, L., … Zambetti, M. (2019). Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: A patient-level meta-analysis of 37,298 women with early breast cancer in 26 randomized trials. Lancet, 393(10179), 1440-1452.
[4] McGehee, C., & Mori, Y. (2024). A mathematical framework for comparison of intermittent versus continuous adaptive chemotherapy dosing in cancer. npj Syst. Biol. Appl., 10(1), 140.
[5] Norton, L., Simon, R., Brereton, H.D., & Bogden, A.E. (1976). Predicting the course of Gompertzian growth. Nature, 264(5586), 542-545.
[6] Simon, R., & Norton, L. (2006). The Norton-Simon hypothesis: Designing more effective and less toxic chemotherapeutic regimens. Nat. Clin. Pract. Oncol., 3(8), 406-407.
[7] Skipper, H.E., Schabel Jr., F.M., & Wilcox, W.S. (1964). Experimental evaluation of potential anti-cancer agents. XIII. On the criteria and kinetics associated with “curability” of experimental leukemia. Cancer Chemother. Rep., 35, 1-111.
[8] Swan, G.W., & Vincent, T.L. (1977). Optimal control analysis in the chemotherapy of IgG multiple myeloma. Bull. Math. Biol., 39(3), 317-337.
[9] Smith, L.A., Cornelius, V.R., Plummer, C.J., Levitt, G., Verrill, M., Canney, P., & Jones, A. (2010). Cardiotoxicity of anthracycline agents for the treatment of cancer: Systematic review and meta-analysis of randomized controlled trials. BMC Cancer, 10, 337.
[10] Von Hoff, D.D., Layard, M.W., Basa, P., Davis Jr., H.L., Von Hoff, A.L, Rozencweig, M., & Muggia, F.M. (1979). Risk factors for doxorubicin-induced congestive heart failure. Ann. Intern. Med., 91(5), 710-717.
[11] Zhang, J., Cunningham, J.J, Brown, J.S., & Gatenby, R.A. (2017). Integrating evolutionary dynamics into treatment of metastatic castrate-resistant prostate cancer. Nat. Commun., 8, 1816.
About the Author
Cordelia McGehee
Internal medicine physician and postdoctoral fellow, University of Pennsylvania
Cordelia McGehee is a practicing internal medicine physician and postdoctoral fellow at the University of Pennsylvania. Her research is in cancer therapeutics with a focus on mathematical modeling of pharmacodynamics and cancer evolution.
Related Reading
Stay Up-to-Date with Email Alerts
Sign up for our monthly newsletter and emails about other topics of your choosing.
