
The Hemodynamic Impact of Medial Arterial Calcification
Medial arterial calcification (MAC) is a vascular disorder that is characterized by the precipitation and crystallization of calcium phosphate within the medial layer of an artery [6]. This disorder is triggered by a breakdown in calcium phosphate homeostasis, which leads to significant mineralization and progressive destruction of an artery’s medial layer. By employing a novel, one-dimensional (1D) hemodynamics simulation, we found that a drop in systolic pressure along a calcified artery is a primary hemodynamic signature of MAC. Such an outcome contrasts sharply with healthy, compliant arteries, where systolic pressure typically amplifies as the pulse wave propagates downstream [3] (see Figure 1).
A major consequence of MAC is arterial stiffening; wherein calcified arteries dilate less under physiological pressure and present a smaller functional lumen area when compared to healthy arteries. This reduced area increases the vessel's impedance, which causes a diminished blood flow rate and could possibly contribute to chronic conditions like limb-threatening ischemia. The hemodynamic signature is obscured by other physiological factors that are associated with MAC. More specifically, both increased peripheral resistance from arteriole closures and “positive remodeling”—an age-related enlargement of the artery's unpressurized lumen—increase the systolic pressure at the arterial outlet, which counteracts or masks the pressure drop from calcification alone [3].
Core Hemodynamic Changes in Calcified Arteries
Our study identifies fundamental differences in blood flow between healthy and calcified arteries that are primarily driven by changes in arterial wall stiffness. A key finding is the differential behavior of systolic pressure along the artery. Healthy arteries normally exhibit systolic pressure amplification, where the distal systolic pressure \((\textrm{Pd})\) is greater than the proximal systolic pressure \((\textrm{Pa}), \) resulting in \(\textrm{Pd}/\textrm{Pa} > 1\) [2]. However, calcified arteries experience a drop in systolic pressure due to the greater impedance that is associated with stiffer arteries, so that \(\textrm{Pd}/\textrm{Pa} < 1,\) (see Figure 1). This outcome is analogous to an electrical resistor that has a larger potential difference across a component with a higher impedance.
![<strong>Figure 1.</strong> Medial arterial calcification alters blood flow, reducing the systolic pressure at the outlet \((Pd)\) relative to the inlet \((Pa).\) In a heathy artery, the outlet systolic pressure can be the same or exceed that of the inlet. Figure adapted from [3].](/media/pdge2qgk/figure1.jpg)
Our simulations reveal a critical paradox regarding lumen size and its impact on blood flow. Ex-vivo arterial cross-sections indicate that unloaded calcified arteries often have larger lumens than unloaded healthy arteries because they are generally older (and therefore larger). But since a calcified artery is stiffer than its healthy counterpart, it exhibits very little pulsatility and hardly dilates under physiological pressures. Under these conditions, the compliant healthy artery achieves a larger in-vivo lumen area, while the calcified artery’s lumen barely changes from its unloaded state. The smaller, functional lumen in calcified arteries results in increased impedance, which leads to a reduced flow rate and could cause decreased peripheral tissue perfusion.
Simulation Methodology
We employed an in-silico approach and used a 1D hemodynamics simulation to model blood flow in a 40-centimeter, tapered femoral-popliteal artery. The model utilized paired partial differential equations to represent conservation of the fluid's mass and momentum [1]. Our method for determining the pressure-area relationship is particularly noteworthy. Instead of relying on an empirical formula, we derived this relationship from a hyperplastic model of the arterial wall that incorporated the mechanical properties of a neo-Hookean solid reinforced with two families of collagen fibers [5]. We prescribed boundary conditions at the inlet and outlet. At the inlet, a time-pressure waveform served as the driving input. At the outlet, a three-component Windkessel model [4] simulated the post-arterial peripheral circulation, allowing us to model increased peripheral resistance via simulated arteriole closures.
Analysis of Competing and Compounding Factors
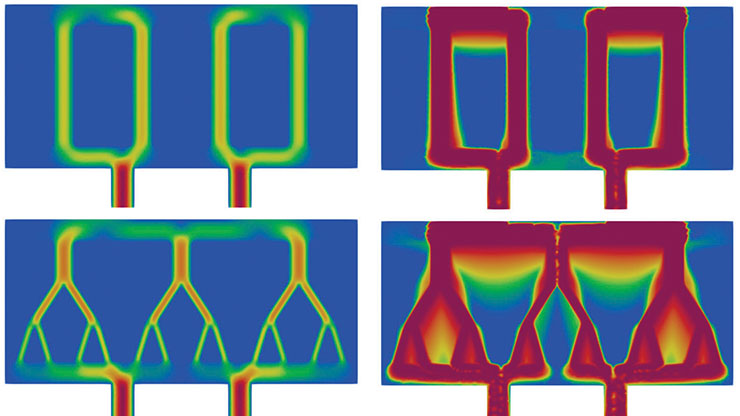
Because the hemodynamic impact of MAC does not solely stem from calcification, our simulation explored arterial stiffening’s interactions with other common physiological changes [3]. Increasing the degree of calcification \((\lambda)\) while keeping other factors constant yields a greater drop in systolic and mean pressure difference, a shrinking of the mean lumen areas at the inlet and outlet, and an overall decrease in outlet flow rate. Furthermore, peripheral resistance rises as the fraction of closed arterioles \((s)\) increases. This result causes systolic and mean pressures at the outlet to increase, thus offsetting the pressure drop from calcification. Meanwhile, closed arterioles also decrease the mean flow rate to compound the effect of calcification. Figure 2 illustrates the opposing effects of increasing the degree of calcification \((\lambda)\) and increasing the fraction of closed arterioles \((s)\) on the systolic pressure difference \((\Delta_{s}) \) between the inlet and outlet.
![<strong>Figure 2.</strong> Increasing the degree of calcification \((\lambda)\) and the fraction of closed arterioles \((s)\) have opposite effects on systolic pressure difference \((\Delta_{s})\) at the inlet and outlet. The characteristic pressure drops arising from calcification can be completely offset or even reversed by high peripheral resistance, masking the presence of MAC. Potential pathways for disease progression are labeled A, B and C. Figure adapted from [3].](/media/zespqs1p/figure2.jpg)
The progression of MAC can follow different pathways depending on the interplay of these factors. If arterial closures and calcification occur together, the systolic pressure will likely not change much between the inlet and outlet (path A in Figure 2). If substantial calcification occurs before significant arteriole closures, a steep drop in outlet systolic pressure ensues (relative to the inlet), followed by a potential recovery as peripheral resistance increases (path B in Figure 2). If arterial closures occur before calcification, the outlet systolic pressure will presumably increase and then decrease (path C in Figure 2).
We also simulated the arteries of older patients whose vessels are stiffer, larger, and more pressurized, since hypertension correlates with age. To do so, we increased the unpressurized inlet radius and driving pressure. These changes increased the outlet systolic pressure, the inlet-outlet systolic pressure difference, and the mean outflow rate, effectively counteracting the effects of calcification and making the vessel behave in a more hydrodynamically healthy manner.
Clinical Applications
Our findings have significant implications for the diagnosis and understanding of MAC. A drop in systolic pressure along an artery is a common indicator of calcification and a potential diagnostic marker. However, the competing effects of increased peripheral resistance and positive remodeling mask this signature and complicate its clinical utility. Therefore, the hemodynamic state of a patient’s artery depends on the complex interplay and timing of these factors.
Our results challenge the standard interpretation of the ankle-brachial index (ABI), a common diagnostic tool for MAC that calculates the ratio of the blood pressure at a patient’s ankle to the blood pressure at their arm. In current practice, an ABI that is greater than \(1.4\) is an internationally recognized marker for MAC [7]. This high threshold is thought to indicate elevated systolic pressure at the ankle compared to the arm. However, our simulations predict that the intra-arterial systolic pressure in a calcified, lower-extremity artery should be reduced instead of elevated. We believe that a mechanical artifact is responsible for the high, clinically measured ABI in calcified arteries. A stiff, calcified artery resists compression by a pressure cuff and requires a much higher external pressure for occlusion. An inflated cuff reading thus occurs because of a non-occlusive arterial wall rather than a high fluid pressure at the ankle.
Ultimately, our work seeks to improve overall understanding of hemodynamics in calcified arteries to improve future disease diagnoses and treatments. For more information, please check out an accompanying video titled “How Stiff Arteries Kill.”
Kun Gou delivered a contributed presentation on this research at the Third Joint SIAM/CAIMS Annual Meetings, which took place in Summer 2025 in Montréal, Québec, Canada.
References
[1] Alastruey, J., Parker, K.H., Peiró, J., & Sherwin, S.J. (2009). Analysing the pattern of pulse waves in arterial networks: A time-domain study. J. Eng. Math., 64(4), 331-351.
[2] Avolio, A.P., Van Bortel, L.M., Boutouyrie, P., Cockcroft, J.R., McEniery, C.M., Protogerou, A.D., … Smulyan, H. (2009). Role of pulse pressure amplification in arterial hypertension: Experts’ opinion and review of the data. Hypertension, 54(2), 375-383.
[3] Fok, P.-W., Gou, K., Myers, B., & Lanzer, P. (2025). Impact of medial calcification on arterial mechanics and haemodynamics. J. Physiol., 603(11), 3341-3355.
[4] Formaggia, L., Lamponi, D., Tuveri, M., & Veneziani, A. (2006). Numerical modeling of 1D arterial networks coupled with a lumped parameters description of the heart. Comput. Methods Biomech. Biomed. Engin., 9(5), 273-288.
[5] Jadidi, M., Sherifova, S., Sommer, G., Kamenskiy, A., & Holzapfel, G.A. (2021). Constitutive modeling using structural information on collagen fiber direction and dispersion in human superficial femoral artery specimens of different ages. Acta Biomater., 121, 461-474.
[6] Lanzer, P., Hannan, F.M., Lanzer, J.D., Janzen, J., Raggi, P., Furniss, D., … Hilaire, C.S. (2021). Medial arterial calcification: JACC state-of-the-art review. J. Am. Coll. Cardiol., 78(11), 1145-1165.
[7] Rac-Albu, M., Iliuta, L., Guberna, S.M., & Sinescu, C. (2014). The role of ankle-brachial index for predicting peripheral arterial disease. Maedica, 9(3), 295-302.
About the Authors
Pak-Wing Fok
Professor, University of Delaware
Pak-Wing Fok is a professor of mathematics at the University of Delaware. His research interests are in cardiovascular modeling, arterial mechanics, and parameter inference.
Kun Gou
Associate professor, Texas A&M University-San Antonio
Kun Gou is an associate professor in the Department of Computational, Engineering, and Mathematical Sciences at Texas A&M University-San Antonio. His research is interdisciplinary, and mainly includes modeling of soft tissues in tubular organs, model computation, and data science.
Stay Up-to-Date with Email Alerts
Sign up for our monthly newsletter and emails about other topics of your choosing.
