
Can a Virus Treat Cancer?
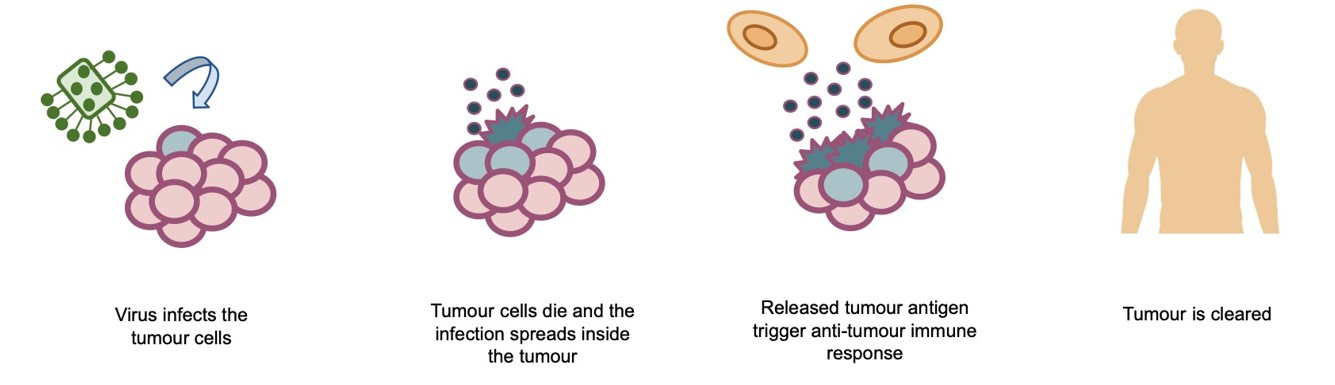
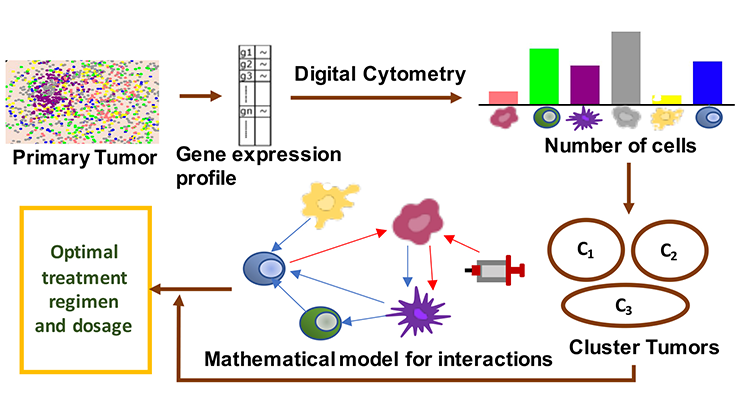
Despite the powerful therapies developed over the past several decades—from chemotherapy to precision-targeted drugs—cancer is still among the leading causes of death worldwide [7] and one of the most formidable challenges in modern medicine [6]. One particularly innovative approach to treat cancer is oncolytic virotherapy (OVT), which uses naturally occurring or genetically engineered viruses to preferentially infect and destroy cancer cells while sparing healthy tissue [3]. These viruses act through dual mechanisms; they directly lyse (break open) tumor cells while simultaneously stimulating the immune system (see Figure 1), thus making them a promising frontier in cancer immunotherapy [4].
Oncolytic viruses can do far more than act as cytotoxic agents [2], they can “prime” the immune system by converting otherwise immunologically unresponsive tumors into immune-responsive ones [1]. Despite this promise, major questions remain: How should viral therapies be scheduled? What is the optimal way to combine them with immune-boosting treatments such as chimeric antigen receptor (CAR) T-cell therapy? How can these complex strategies be optimized without relying solely on costly and time-consuming clinical trials?
This is where mathematics provides a powerful lens. By integrating biological insight with mathematical modeling, researchers can systematically explore treatment schedules, predict therapy outcomes, and identify optimal strategies. Such interdisciplinary approaches offer a promising pathway toward understanding how oncolytic viruses and immune therapies can be optimized to achieve more effective cancer control.
Mathematical Models: A Virtual Laboratory
We developed a mathematical model that consists of a system of ordinary differential equations to describe how populations of tumor cells, viruses, and immune cells interact over time [5]. While our model is not meant to replace experiments, it can serve as a virtual laboratory where scientists can simulate and refine ideas that might be difficult to test directly in early stages of experimentation.
At its core, our model improves upon conventional virus-tumor interaction models by incorporating variables for immune response and multiple treatments. With the use of these models we examined:
- Virus parameters, including the burst size (i.e., the number of new viruses produced when an infected tumor cell lyses).
- Immune dynamics, acknowledging that immune cells play both supportive and antagonistic roles in virus-tumor interactions.
- Scheduling effects, exploring how the timing, dosage, and sequence of viral injections affect overall outcomes.
- Combination therapies, including the integration of immune therapies such as CAR T-cell therapy, which engineer a patient’s T-cells to target cancer.
Because clinical data for these combinations are limited—especially across different cancer types and experimental settings—our findings are qualitative rather than quantitatively predictive; even so, the results pave a conceptual path to strategies worth investigating experimentally.
Timing Matters: What the Simulations Reveal
One of the most striking insights from our study was the critical role of timing. Our analysis revealed that the schedule of viral injections—specifically when and how often a virus is administered—can create dramatically different therapeutic outcomes. Rather than applying treatments uniformly, administering targeted doses during times when the immune response was most receptive or when tumor dynamics were most vulnerable substantially improved tumor control in the simulation. In several trials, one strong viral dose followed by carefully spaced booster injections produced far more favorable outcomes than evenly distributed dosing schedules.
This is not merely a mathematical artifact. In real biological systems, viruses and immune cells engage in a dynamic competition: oncolytic viruses must infect and replicate within tumor cells before they are cleared by the immune system, while immune cells require sufficient exposure to viral antigens in order to mount an effective antitumor response. Optimizing the timing of these interactions can therefore determine whether a therapy stalls or succeeds.
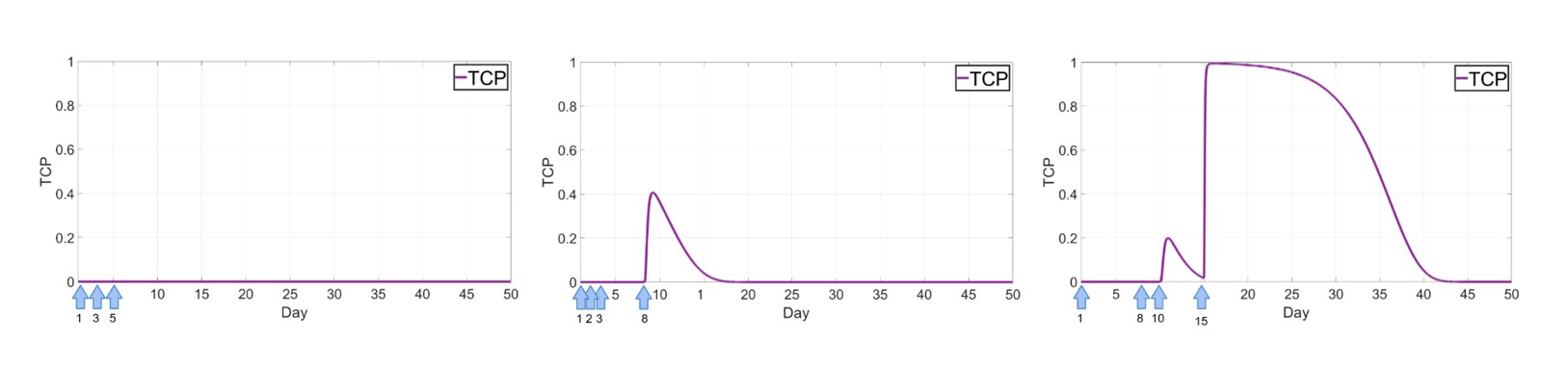
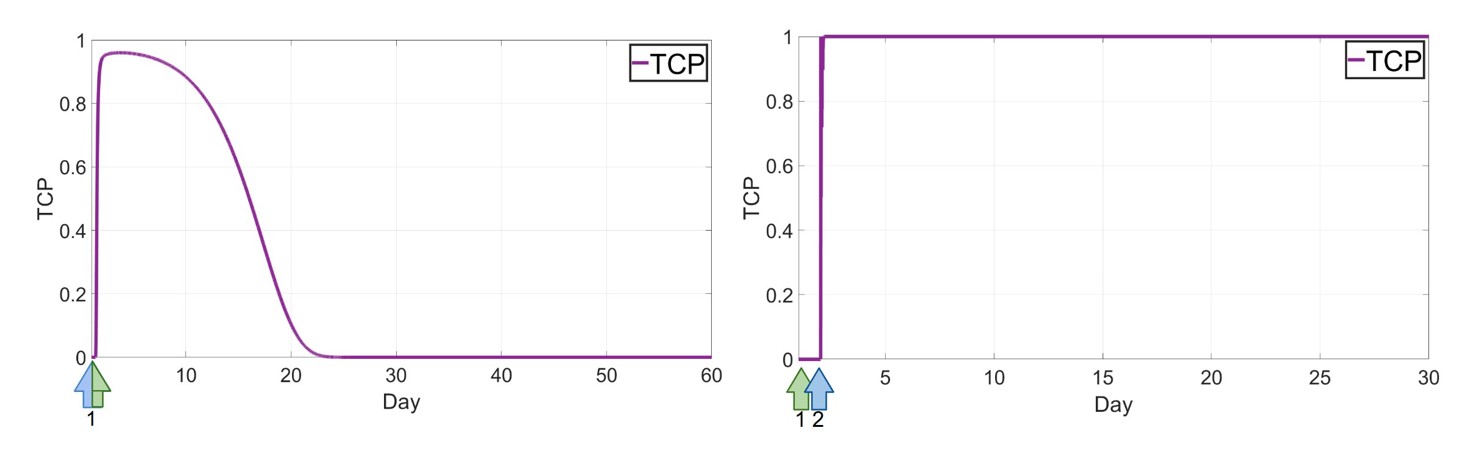
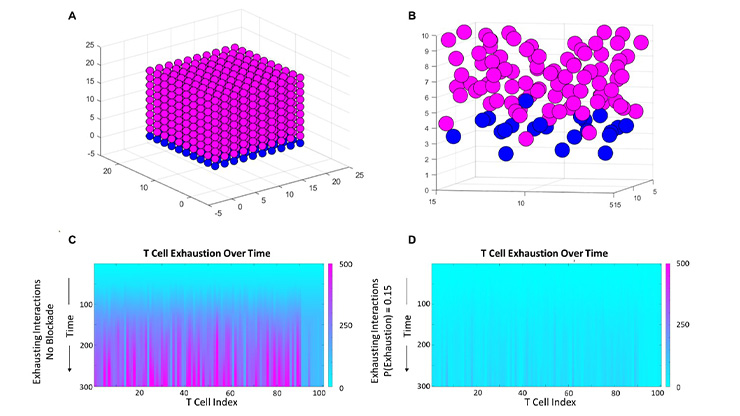
To quantify treatment success in our simulations, we utilize tumor control probability (TCP), a standard measure used to determine the probability that a treatment strategy successfully controls or eliminates a tumor. A TCP value close to one indicates a high likelihood of success, while values near zero correspond to poor therapeutic outcomes. By comparing TCP across different treatment schedules, we can directly evaluate the effectiveness of competing strategies. As illustrated in Figure 2, optimized timing and dosing strategies lead to TCP curves that rise toward one.
Combination Therapy: More Than the Sum of Its Parts
One of the most promising features of OVT is its potential to be combined with other immunotherapies, particularly immune-modulating treatments such as CAR T-cell therapy. In our study, we investigated how strengthening the immune response in a way that complements viral activity can shift the system toward sustained tumor suppression.
Although CAR T-cell therapy has achieved remarkable success in certain blood cancers, its effectiveness in solid tumors has been limited [8]. One reason for this is the highly immunosuppressive tumor microenvironment, which can prevent immune cells from fully activating and persisting. OVT offers a potential solution: by infecting and lysing tumor cells, they can disrupt this suppressive environment and expose tumor antigens to immune recognition. Our mathematical framework suggests that carefully chosen schedules and treatment combinations can significantly amplify this synergy, demonstrating that combination therapy can be more effective than either treatment alone.
Among all strategies we tested, the most successful was a combined OVT and CAR T-cell regimen. While the simultaneous administration of both therapies produced a substantial improvement over single-treatment approaches, the most effective outcome emerged when both treatments were delivered within one or two days, starting with CAR-T therapy and followed by OVT. In this scenario, the initial CAR T-cell infusion rapidly reduces the tumor burden, while the oncolytic virus acts as an immune booster, reinforcing and sustaining the antitumor immune response. This cooperative mechanism—where immune cells weaken the tumor and viral therapy amplifies immune activation—captures the central promise of combination immunotherapies and highlights their potential for treating solid tumors more effectively.
From Virtual Insight to Real-World Impact
The true impact of this work is not to deliver a ready-to-use treatment protocol, but to inform the work of experimental biologists, translational researchers, and clinicians who design and test therapies. The models explain why timing and scheduling matter and identify which therapeutic strategies are most likely to succeed, thereby helping researchers prioritize the most promising experiments.
Looking Ahead
No model is perfect, and we acknowledge the limitations of this work. The reliance on parameter sets from different cancers and experimental setups means that the results are not yet validated quantitatively across specific cancers.
Yet, progress is accelerating. As more experimental and clinical data become available, especially from trials involving oncolytic viruses and immune therapies, models can be calibrated and refined. Our mathematical toolkit also continues to expand, with techniques from optimization, data assimilation, and machine learning becoming integrated with classical models to further enhance predictive power and treatment personalization.
Negar Mohammadnejad delivered a minisymposium presentation on this research at the Third Joint SIAM/CAIMS Annual Meetings (AN25), which took place last summer in Montréal, Québec, Canada. She received funding to attend AN25 through a SIAM Early Career Travel Award. To learn more about Early Career Travel Awards and submit an application, visit the online page.
References
[1] Garofalo, M., Pancer, K.W., Wieczorek, M., Staniszewska, M., Salmaso, S., Caliceti, P., Kuryk, L. (2022). From immunosuppression to immunomodulation - Turning cold tumours into hot. J. Cancer, 13(9), 2884-2892.
[2] Jafari, M., Kadkhodazadeh, M., Shapourabadi. M.B., Goradel, N.H., Shokrgozar, M.A., Arashkia, A., ... Sharifzadeh, Z. (2022). Immunovirotherapy: The role of antibody based therapeutics combination with oncolytic viruses. Front. in Immunol., 13.
[3] Lin, D., Shen, Y., & Liang, T. Oncolytic virotherapy: Basic principles, recent advances and future directions. Signal Transduct. Target Ther., 8(1):156.
[4] Marelli, G., Howells, A., Lemoine, N.R., & Wang, Y. (2018). Oncolytic viral therapy and the immune system: A double-edged sword against cancer. Front. Immunol., 9, 866.
[5] Mohammadnejad, N. & Hillen, T. (2026). Qualitative optimization of oncolytic virotherapy and immune therapy combination treatments[J]. MBE, 23(2), 388-420.
[6] World Health Organization. (2024). Global cancer burden growing, amidst mounting need for services. Retrieved from https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing-amidst-mounting-need-for-services.
[7] World Health Organization. (2025). Cancer. Retrieved from https://www.who.int/news-room/fact-sheets/detail/cancer.
[8] Zhu, J., Zhou, J., Tang, Y., Huang, R., Lu, C., Qian, K., ... Chen, S. (2025). Advancements and challenges in CAR-T cell therapy for solid tumors: A comprehensive review of antigen targets, strategies, and future directions. Cancer Cell Int., 25(1):313.
About the Author
Negar Mohammadnejad
Ph.D. candidate, University of Alberta
Negar Mohammadnejad is a Ph.D. candidate at University of Alberta. Her research interests include mathematical biology, partial differential equations (PDEs), and cancer cell modelling. Her work focuses on developing and analyzing mathematical models to study cancer therapies and to better understand mechanisms that could improve the effectiveness of different treatment strategies.

Stay Up-to-Date with Email Alerts
Sign up for our monthly newsletter and emails about other topics of your choosing.
